Structural proof. Imaged in 3D, measured in cubic centimeters, read by two doctors on the same scan. No named patients, no promises. The number does the talking.
When structure changes, it shows in more than one place. The airway opens, the arch widens, the body re-stacks, three measured changes on one de-identified patient.
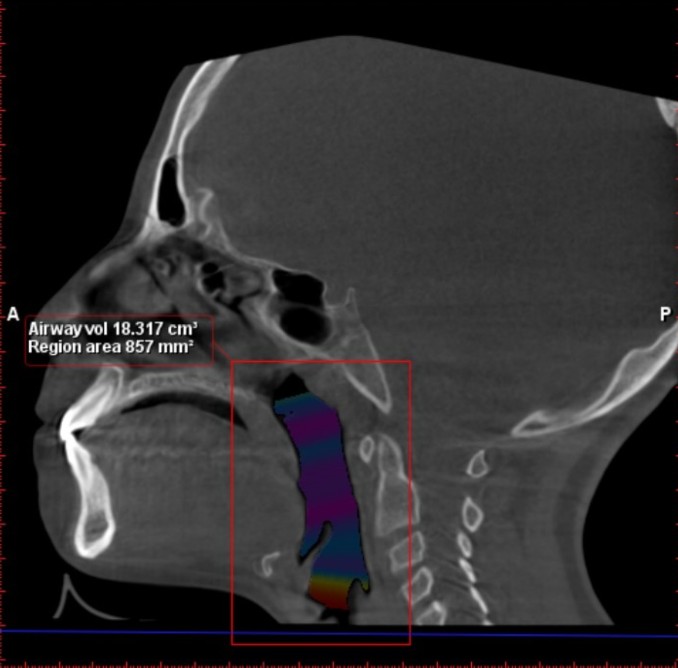
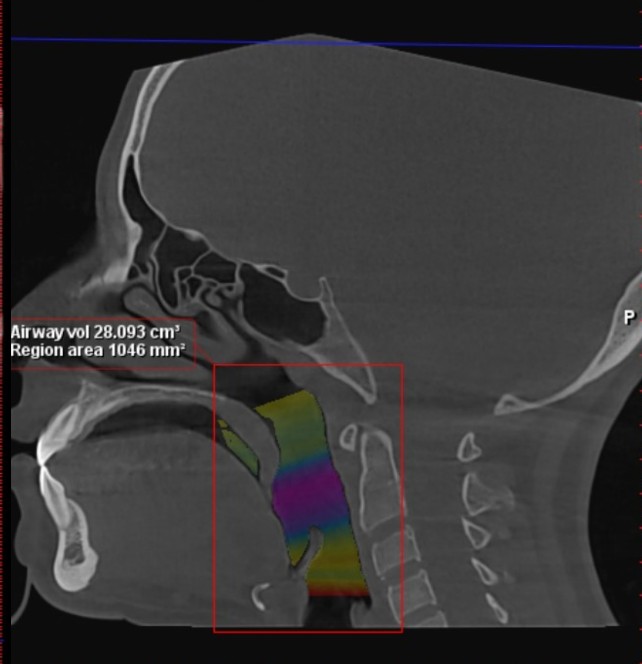
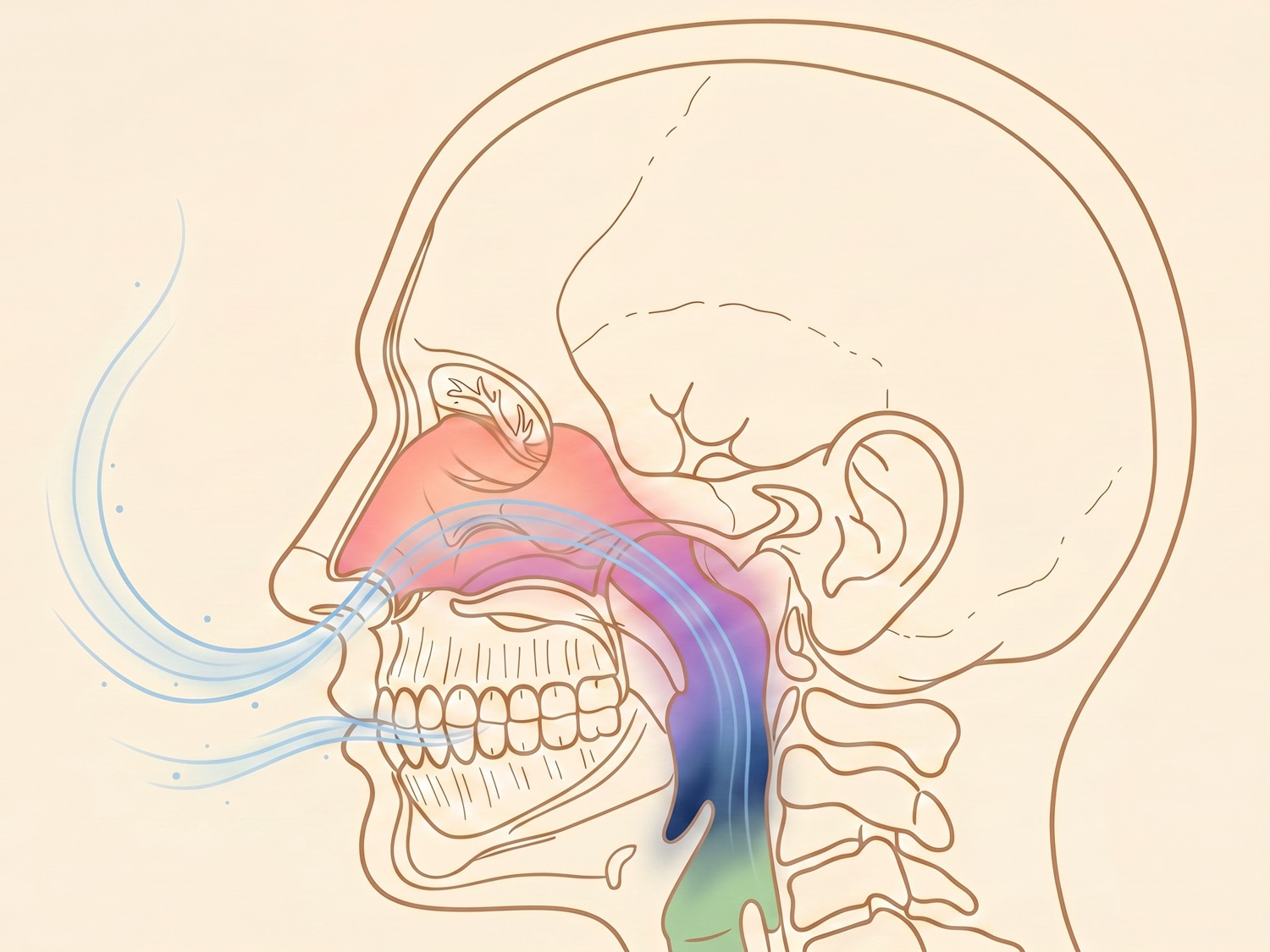
The airway, in volume
The space available to breathe, measured
Sagittal 3D cone-beam CT. The colored channel is the airway, reconstructed and measured in cubic centimeters.
De-identified, education only. Individual anatomy and results vary.
Airway volume increased from 18.32 to 28.00 cubic centimeters, a 53 percent increase.
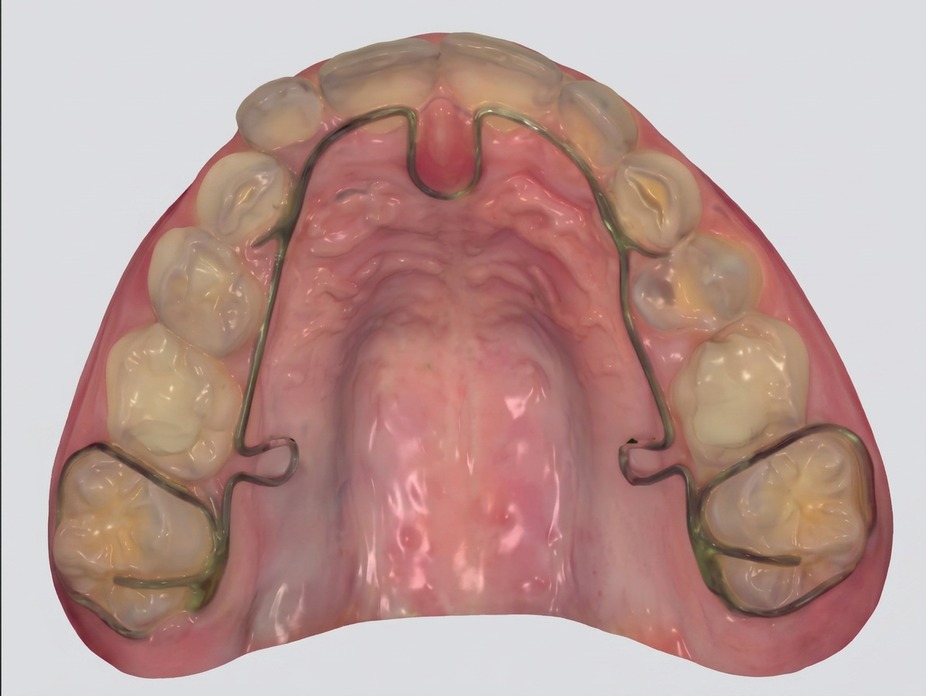
The arch, in three dimensions
A wider palate to breathe and rest the tongue in
3D intraoral scans of the upper and lower arch. The same arch, redeveloped wider, with more room behind the teeth.
BeforeNarrower arch, crowded biteAfterWider palate, more tongue room
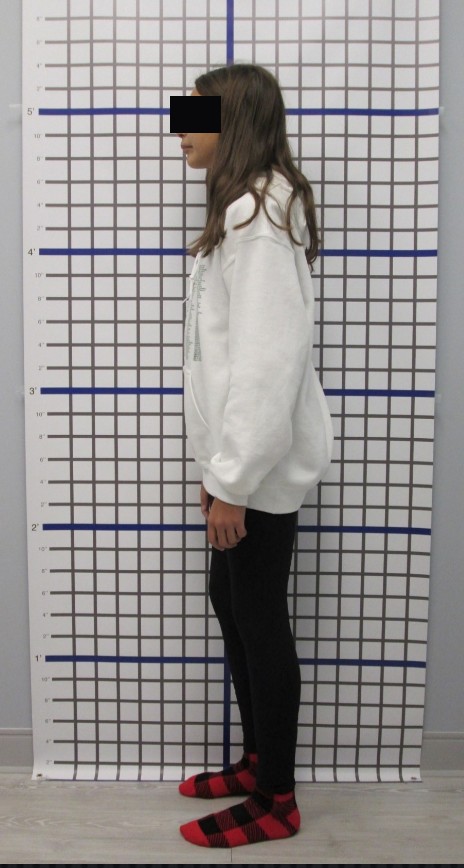
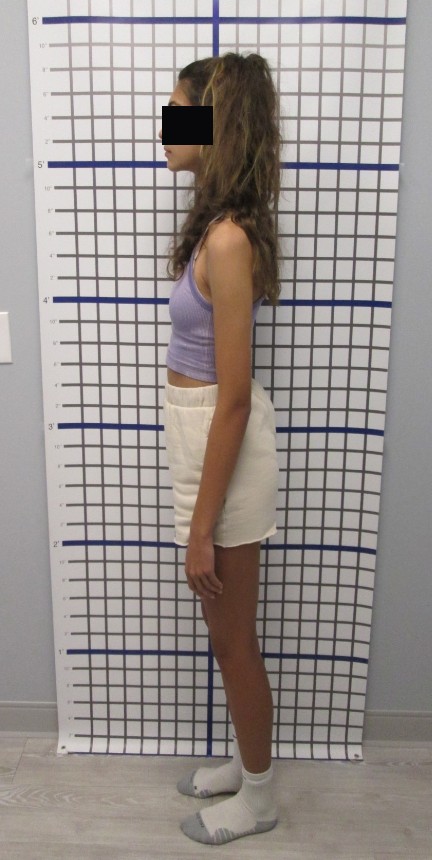
The body, on a grid
A frame that re-stacks once it can breathe
Read against a plumb-line grid wall. As the airway opens, the head and shoulders tend to come back over the spine.
BeforeForward head, beforeAfterRe-stacked over the spine, after
Procedures don’t heal patients. Physiology does.
De-identified imagery from one patient, shown for education. Faces and names withheld. Non-diagnostic, and not a typical, expected, or guaranteed result. Individual anatomy and results vary.
Why we can measure it
The same anatomy, from every angle.
A flat X-ray gives one shadow. A 3D scan lets two doctors read the same structure in volume, cross-section, and context, so proof becomes a number.
In three dimensions
Volume, not a shadow
The space available to breathe through
Reconstructed in 3D, then measured in cm³
In cross-section
The narrowest point, visible
A slice through the same airway
Where the tightest points become measurable
In context
Muscle and soft tissue
The structures around the airway
Jaw and tongue posture, read together
Patient stories
The proof, in their own words.
A few of the people who came in for one read. Hover to unmute.
Patient of AlignessPatient of AlignessPatient of Aligness
The second lens
The airway is read alongside what the eyes reveal.
Aligness reads systems, not symptoms. The oxygen the airway carries reaches the smallest vessels, and the eye is one of the few places those vessels are seen directly. The scan and the eye read the same person from two angles.
The eyeWhere small vessels and oxygen delivery can be observed
The airwayWhere that oxygen is carried in and measured on CBCT
One personTwo doctors, one read, the whole picture together
Clinical cases
What neither specialty sees alone.
Dental and ophthalmologic care under one roof catches what neither specialty sees alone, a pattern our physicians documented where the mouth and the eye read the same body.
Case 01
A graft stable for nearly six years, then refractory rejection
A corneal transplant stable for nearly 6 years began recurrent rejection that was refractory to standard ophthalmic management for about 2 years. A dental exam found lichen planus.
After targeted oral treatment, the graft cleared and vision reached 20/60 within one month, without changes to ophthalmic therapy.
Case 02
Graft failure with rejection, and an untreated mouth
A corneal transplant with graft failure and recurrent rejection for about 3 years. Dental evaluation found active infection and untreated caries.
Within one month of dental treatment, the graft cleared and vision returned to baseline.
Case 03
Progressive edema that tracked a lost crown
A corneal transplant with progressive edema and recurrent rejection that correlated with the loss of a dental crown and oral neglect.
After crown restoration and resolution of oral inflammation, rejection resolved and vision stabilized within one month.
The clinical note
These cases do not establish causation. They show a pattern we observed, so we now treat oral-health evaluation as a standard part of the workup for refractory graft rejection.
Taught to clinicians
The method other doctors travel to learn.
Dr. Pastouk created Glossodontics®, the method that releases the tongue then redevelops the airway, jaw, and face. The same read he and Dr. Skeens use with you.
Reading the scan togetherPresenting the method
Presented at a clinical conference on airway and integrative care. Shared to illustrate professional standing, not to promise any individual outcome.
Who reads your picture
The credentials behind the room.
Two board-credentialed doctors who read your picture themselves, and together. One makes the hidden structure visible. One reads the whole pattern of airway, oxygen, and what the eyes reveal.
Dr. Vladimir Pastouk, DMD, ND
The structural and airway lens · Creator of Glossodontics®
Airway and biological dentist (DMD, ND)
Creator of Glossodontics®, who presents the method to other clinicians
Refers airway-related sleep concerns to sleep medicine
Dr. Heather Skeens, MD
The eye, oxygen, and whole-body lens
Board-certified ophthalmologist and eye surgeon
Certified functional medicine practitioner
Reads the eye as one integrative, non-diagnostic input, never alone
The proof is structural
Procedures don’t heal patients. Physiology does.
Two doctors read your whole picture, in one room, and give you one honest next step. Consults run online. Patients fly in to be seen.