Glossodontics® is the method Dr. Vladimir Pastouk created and has presented to other doctors. It releases the tongue so the airway, jaw, and face can redevelop, and you breathe through your nose again.
“Still tired after CPAP.” “My labs are normal but I still feel terrible.” If you have lived one of those, the airway is the part almost no one has looked at.

Dr. Pastouk treats the airway as structure, not an afterthought. He created Glossodontics®, the method for redeveloping the airway and the space behind the tongue, and presents it to other clinicians.
He reads the jaw, the palate, the tongue, and the airway you can measure on a 3D CBCT scan, not estimate, alongside Dr. Skeens, in one room.
Fatigue goes to one office, the jaw to another, the labs to a third. No one compares notes. Aligness reads systems, not symptoms, so the airway is read against your whole picture instead of in isolation.
The tongue has a real job: support and widen the palate, drive nasal breathing, and help the face and jaws grow into shape. When it cannot do that job, the effects travel. Glossodontics® works the chain from the start instead of chasing it at the end.
A restricted tongue cannot rest where it should or drive easy nasal breathing. The release frees it to do its real work.
With the tongue freed, the channel at the back of the mouth and throat is given room to open.
The arches can be widened and redeveloped, so the jaw and palate find a calmer, more balanced position.
Nasal breathing and a balanced jaw are the foundation the face and posture have always been built on.
Easier breathing at night may be linked to deeper rest, steadier energy, focus, and mood.
Procedures don’t heal patients. Physiology does.
A plain procedure ends at the cut. Glossodontics® is built around the healing, so the body is supported through recovery, not just released.
One patient’s airway on a 3D CBCT scan, before and after. Not a slogan, a volume you can read straight off the scan.
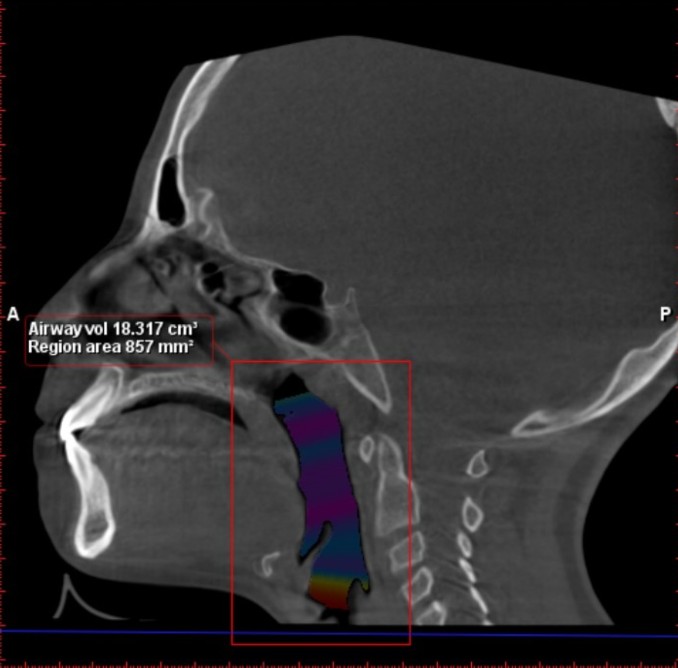 Before
Before
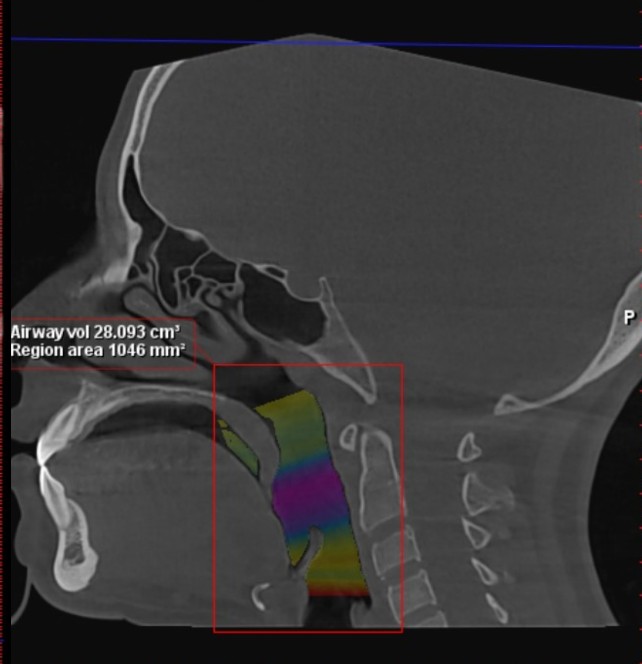 After
After
18.32 28.00 cm³
+53% airway volume
De-identified, education only. Individual anatomy and results vary.
Airway volume increased from 18.32 to 28.00 cubic centimeters, a 53 percent increase.The same structure, finally read in three dimensions rather than guessed.
De-identified 3D CBCT airway-volume comparison, shown for education only. Not a promise of any outcome, not a diagnosis; individual anatomy and results vary.
The airway does not change in isolation. As the arches are redeveloped, the upper and lower jaws are given room they did not have before.
 Before
Before After
After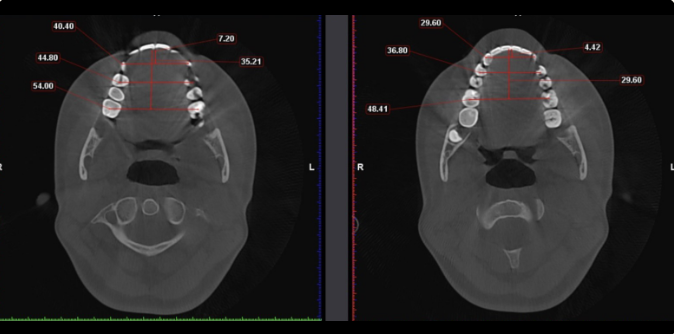 Before
After, widened
Before
After, widened
Grinding and clenching are often the jaw bracing against a tight airway. Give the airway room, and the jaw has less to fight at night.
The shape of the upper arch, the room behind the teeth, and where the tongue can rest all shape how easily you breathe. It is the structural read a standard workup is not trained to make.
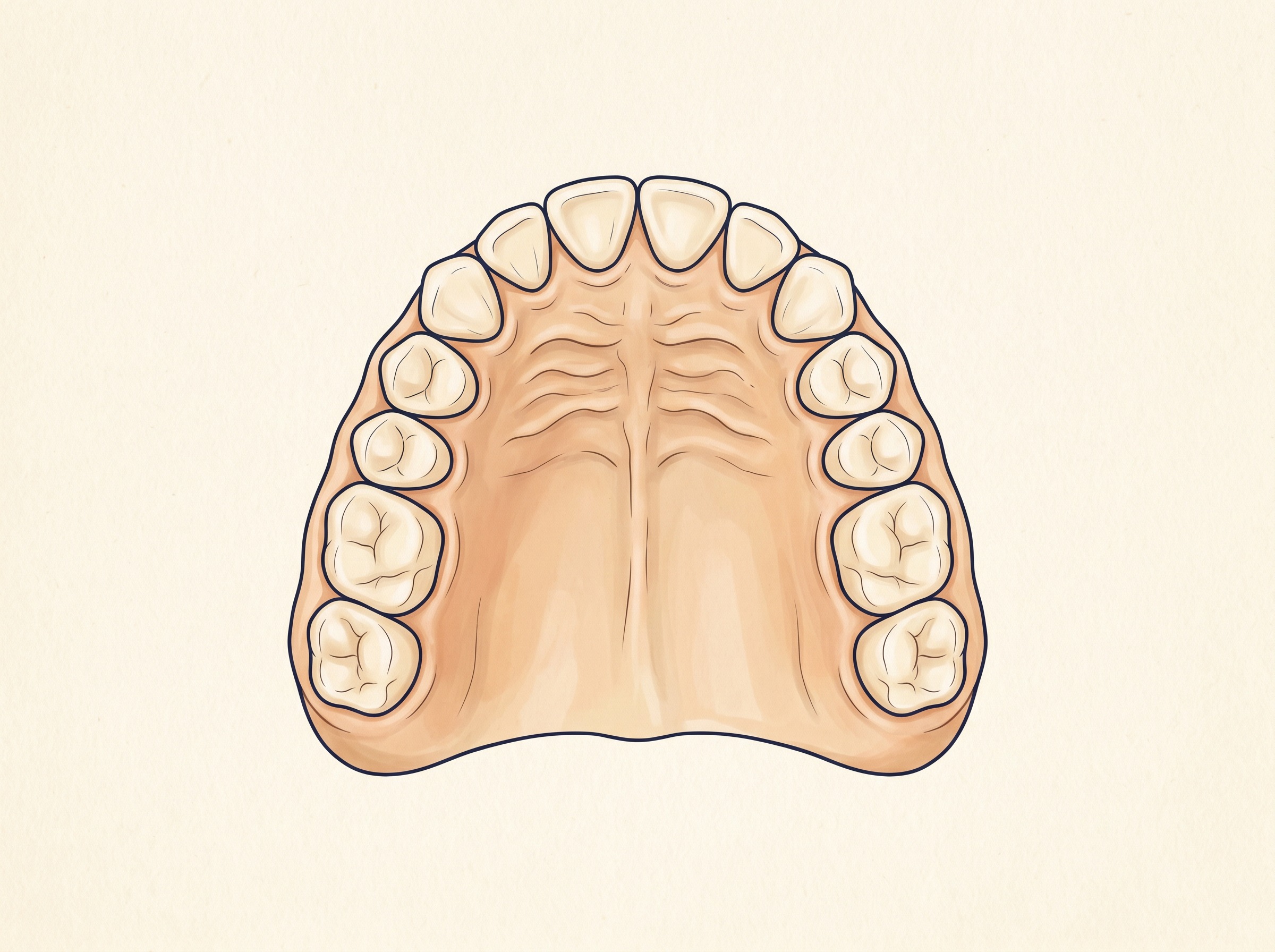
A narrow, crowded arch leaves the tongue no room and crowds the airway behind it. Widen and redevelop the arch, and the tongue, jaw, and airway are given the space they were built to have.
Both doctors present this work to other clinicians at national conferences, under one banner: eye, dental, and functional medicine, read as one body.
These signs usually get treated one at a time, in different offices. Read together, a pattern can emerge.
An honest practice is clear about its edges. So you know exactly what you are applying for, here is where we stand.

Bring your sleep, your energy, and everything you have already tried into one room with two doctors who know how to read them together. You leave with one clear next step.